I have a guest article on Vitamin D written by Joel Dawson, Sport Scientist at Stcke City Football Club. You can follow him on twitter - @joeldawson9
There is a rising awareness about
the value of vitamin D for both health and athletic performance. It is an
essential nutrient, which contributes to bone health, muscle functionality and
calcium regulation in the blood, to name a few. However, contrary to other
vitamins, it is difficult to source and acquire the recommended daily amount
with the principal source of vitamin D from ultraviolet B radiation in sunlight.
The limited availability of naturally occurring vitamin D in dietary foods may
provide a viable argument for the fortification of more foods. Evidence detailing
the physiological importance of vitamin D will be reviewed as well as an
assessment about the readily source availability of the vitamin and needs of
different population groups. Only then can it be argued to whether or not
fortifying different food groups is a logical and obligatory option moving
forward.
Vitamin D has been found to play
an active role in many physiological processes in the body (Ogan and Pritchett
2013). Firstly, Vitamin D is most well known for its active role in osteoclast
activity and absorption of calcium in the intestine (Larsen-Meyer et.al 2010).
An inadequate amount of vitamin D can lead to bone loss and injury because it
has a crucial function in bone growth, density and remodelling (DeLuca 2004).
For example, if infants and children are chronically deficient in vitamin D
then the risk of rickets becomes a progressive and prominent problem (Hollick
et.al 2004). Low status of this vitamin can also impair calcium and phosphorus
homeostasis, resulting in a restricted calcium absorption rate in the small
intestine (Heaney et.al 2003). Metabolic processes, neuromuscular activity and
bone health are compromised when calcium absorption is insufficient, further
stressing the importance of maintaining adequate vitamin D status. The
identification of vitamin D receptor (VDR) sites in an array of tissues within
the body (Holick et.al 2005) is important because VDR regulates hundreds of
gene expression that perform vital bodily functions. Epidemiological evidence
suggests that the VDR is involved in mediating the noncalcemic effects of
vitamin D and could play an imperative role in maintanence of extracellular
health and disease prevention (Grant et.al 2005).
The
desirable intake levels of vitamin D are yet to be fully recognised, with
recommendations differing amongst medical institutions. New guidelines were
released by the Institute of Medicine (IOM) in 2010 recommend children and
adults (0-70 years) to intake 400-600 IU/day with older adults (>70 years)
advised to have 800 IU/day from the diet. Although, clinically it may be an
amount that prevents vitamin D deficiency, it is a recommendation that is
insufficient for fully optimised vitamin D levels (Ginde et.al 2009, Heaney
2008). The Endocrine Society, for example, proposes much higher dietary intake
recommendations in addition to rational sun exposure. The comparison between
the two dietary allowance advocated by the two institutes is exemplified in table
1 below.
Table 1: Recommended
vitamin D intake levels of the IOM vs Endocrine society. Taken from Ogan &
Pritchett (2013)

Table 2: Reference
values for serum 25(OH)D taken from Larson-Mayer et.al 2013

Reaching levels of >32ng/mL
will enhance calcium absorption and it is at this point in which functionality
of vitamin D is efficiently demonstrated (Canell et.al 2008). However, the
greatest benefit of vitamin D is fully appreciated above the optimal threshold with
storage in fat or muscle not occurring if circulating 25(OH)D levels are
>40ng/ml (Cannell et.al 2009). Therefore, advanced processes will require
frequent daily replenishment of vitamin D, a recurrent source that is currently
unattainable from the common diet. This seemingly suggests that the current
recommendation of 600IU per day by the IOM is only designed to prevent clinical
deficiency of <20ng/mL, with higher levels such as 1000IU per day increasing
availability at optimal levels of vitamin D. Holick et.al (2005) has even
estimated values of 3000-5000IUdaily to fully meet the physiological needs of
the body. In terms of toxicity, daily intakes of 10,000IU can take years to
manifest toxic symptoms after extended use (Heaney et al 2008) with no toxicity
incidents reported either from sun overexposure UVB exposure (15minutes can
provide 10,000-20,000IU) (Ogen & Prtichett 2013). Over supplementation
seems to be the feasible cause of intoxication with outdoor workers living near
to the equator only showing levels of around 50ng/mL (Cannell et.al 2008). This
suggests that dietary sources of vitamin D could potentially be optimised
without the risk of toxicity.
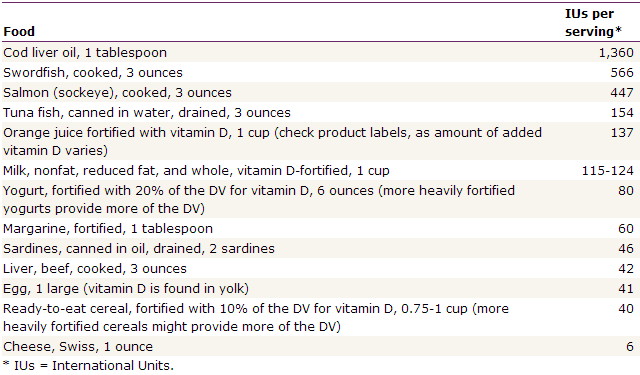
Vitamin D is primarily sourced
from ultraviolet rays triggering synthesis endogenously when the skin is
exposed to sunlight. It is also naturally present is foods such as fatty fish
(salmon, tuna, sardines, mackerel), egg yolks, types margarine and fortified in
products such as milk, orange juice and cereal (Chen et.al 2007) (see table 1
for examples of food and IU’s per serving). However, much of the nutrient value
of dietary vitamin D can be lost within the absorption process, with evidence
showing it to be a process that is 50% efficient (Mahan et.al 2004).
Table 3: Selected Food Sources of
Vitamin D (U.S. Department of
Agriculture, Agricultural Research Service. 2011)
Some population groups have an
emphasis on alternative vitamin D stores. For example, individuals with dark
skin have greater amounts of melanin in the epidermal layer of the skin which
reduces the ability to produce vitamin D from sunlight. A study in 1546 African
women showed that > 40% had deficient levels of vitamin D (Nesby’O’Dell
et.al 2002) with 82% Asian adults in the UK also deficient in the vitamin (Pal
et.al 2003) in the summer months. The need for vitamin D is also more prevalent
in younger populations, the elderly and pregnant women. Approximately 40-100%
of Elderly men and women from the US and Europe for example are said to be
deficient in vitamin D (Holick et.al 2007). Overall, an estimated 1 billion
individuals worldwide are deficient or insufficient in vitamin D levels (Holick
et.al 2007); therefore any solution for increasing daily intakes of vitamin D
should be taken seriously with fortification a viable option given the current
low levels attainable commercially in the diet. However, achieving the recommended daily aim
of 1500-2000IU set by the Endocrine Society is difficult to obtain from food
with fortified products only containing 40-140IU per serving on average (see
table 3).
Vitamin
D and athletic performance is an area of research that is becoming more
prominent. Close et.al (2013a) showed that muscle performance in young UK based
athletes did not improve following either a dose of 20,000IU or 40,000IU over a
12 week period with supplementation not inducing levels above 40ng/mL. However,
a larger study by this study group did show that a daily dose of 5000IU was
more superior in raising levels above 40ng/mL with this daily dose improving
vertical jump height and 10 meter sprint times (Close et.al 2013b), suggesting
that optimal levels of vitamin D can improve the anaerobic concept of
performance. It also worth noting that inadequate vitamin D concentration had a
negative impact on musculoskeletal performance in athletes. Inflammation
markers in endurance athletes have also been associated with low vitamin D status
(Willis et al 2012). The requirements for the athlete will be even greater to
fully optimise stores during times of physical activity to ensure sufficient
stores for increased physiological demands.
After
reviewing the current literature, there is a clear positive influence when daily
intakes of the vitamin lead to optimal serum 25(OH)D levels in the body. The
inadequacy of vitamin D stores is prevalent amongst a high amount of the
population and the need for these optimal stores is also particularly apparent
across children, the elderly, dark skinned individuals and athletes. Although the
primary source of vitamin D comes from sunlight exposure, the ongoing
deficiency exemplifies that suffice levels are not obtained on a daily basis. Therefore,
fortification of more food groups seems a reasonable way to proceed in order to
increase bodily vitamin D stores, in the form of a readily available daily
source. Although larger experimental research exploring the impact of dietary
vitamin D is needed, not even regular intakes 30,000IU for an extended period
of time will manifest the symptoms of toxicity (Heaney et.al 2008). This
indicates that taking in too much vitamin D from the diet will not create a
toxic environment, with the digestion process also nullifying vitamin D
absorption. There is also a rationale to provide a controlled supplementation
to particular groups. Reaching optimal levels of 40ng/mL, will not only meet fundamental
metabolic processes but also ensure extra storage for muscular performance gains.
Although research in this area is its infancy, the performance gain from
optimal vitamin D status is encouraging and should be considered by athletes
and coaches alike.
References
Cannell, J.J.; Hollis, B.W.; Sorenson, M.B.; Taft, T.N.; Anderson,
J.J.B. Athletic performance and vitamin D. Med. Sci. Sport Exerc. 2009,
41, 1102–1110.
Chen, T.C.; Chimeh, F.; Zhiren, L.; Mathieu, J.; Person, K.S.;
Zhang, A.; Holick, M.F. Factors that influence the cutaneous synthesis and
dietary sources of vitamin D. Arch. Biochem. Biophys. 2007, 460,
213–217.
Close, G.L.; Leckey, J.; Patterson, M.; Bradley, W.; Owens, D.J.;
Fraser, W.D.; Morton, J.P. The effects of vitamin D3 supplementation on serum
total 25(OH)D concentration and physical performance: A randomised
dose-response study. Br. J. Sports Med. 2013, in press.
Close, G.L.; Russel, J.; Cobley, J.N.; Owens, D.J.; Wilson, G.;
Gregson, W.; Fraser, W.D.; Morton, J.P. Assessment of vitamin D concentration
in non-supplemented professional athlettes and healthy adults during the winter
months in the UK: Implications for skeletal muscle function. J. Sports Sci. 2013,
31, 344–353.
Cannell, J.J.; Hollis, B.W. Use of vitamin D in clinical practice.
Altern. Med. Rev. 2008, 13, 6–20.
DeLuca, H.F. Overview of general physiologic features and
functions of vitamin D. Am. J. Clin. Nutr. 2004, 80,
1689–1696.
Ginde, A.A.; Liu, M.C.; Camargo, C.A. Demographic differences and
trends of vitamin D insufficiency in the U.S. population, 1988–2004. Arch.
Intern. Med. 2009, 169, 626–632.
Grant, W.B.; Holick, M.F. Benefits and requirements of vitamin D
for optimal health: a review. Altern Med
Rev. 2005, 10, 94-111.
Heaney, R.P.; Dowell, M.S.; Hale, C.A.; Bendich, A. Calcium
absorption varies within the reference range for serum 25-hydroxyvitamin D. J Am Coll Nutr. 2003, 22, 142-146
Heaney, R.P. Vitamin D in health and disease. Clin. J. Am. Soc.
Nephrol. 2008, 3, 1535–1541.
Holick, M.F. Sunlight and vitamin D for bone health and prevention
of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004, 80, 1678S-1688S.
Holick, M.F. The vitamin D epidemic and its health consequences. J.
Nutr. 2005, 135, 2739S–2748S.
Holick, M.F. 2007.Vitamin D deficiency. N Engl J Med. 2007, 357,
266-81.
Institute of Medicine of the National Academies. Dietary
Reference Intakes for Calcium and Vitamin D; Catharine Ross, A., Taylor,
C.L., Yaktine, A.L., Eds.; The National Academy of Sciences: Washington, DC,
USA, 2011.
Larsen-Meyer, D.E.; Willis, K.S. Vitamin D and athletes. Curr.
Sports Med. Rep. 2010, 9, 220–226.
Larson-Mayer, D.E.;
Burke, L.M.; Stear, S.J.; Castell L.M. A–Z of
nutritional supplements: dietary supplements, sports nutrition foods and
ergogenic aids for health and performance: Part 40. Br J Sports Med. 2013, 47, 118-120.
Mahan, L.K.; Escott-Stump, S. In Krause’s Food, Nutrition and
Diet Therapy, 11st ed.; Gallagher, M.G., Ed.; Elsevier: Philadelphia, PA,
USA, 2004, 83–88.
Nesby-O’Dell, S.; Scanlon, K.S.; Cogswell, M.E.; Hypovitaminosis D
prevalence and determinants among African American and white women of
reproductive age: third National Health and Nutrition Examination Survey,
1988-1994. Am J Clin Nutr. 2002, 76:187-192.
Ogen, D.; Pritchett.K. Vitamin D and the athlete: risks, recommendations,
and benefits. Nutrients. 2013, 5, 1856-1868
Pal, B.R; Marshall T.; James C.; Shaw N.J. Distribution analysis
of vitamin D highlights differences in population subgroups: preliminary observations
from a pilot study in UK adults. J
Endocrinol. 2003, 179, 119-129
Willis, K.S.; Peterson, N.J.; Larson-Meyer, D.E. Should we be
concerned about the vitamin D status of athletes? Int. J. Sport Nutr. Exerc.
Metab. 2008, 18, 204–224.